 Sure, this is the fifth post of 2016 – and its July – however there is a good reason for it. I continue to be an on the field athletic trainer, I continue to educate on concussion, I continue to be active on Twitter but more importantly I am concentrating more on being a father and husband. Blogging ain’t easy, folks; let’s be honest the coverage of concussion has blossomed well since 2009 when this blog started.
Sure, this is the fifth post of 2016 – and its July – however there is a good reason for it. I continue to be an on the field athletic trainer, I continue to educate on concussion, I continue to be active on Twitter but more importantly I am concentrating more on being a father and husband. Blogging ain’t easy, folks; let’s be honest the coverage of concussion has blossomed well since 2009 when this blog started.
All of that being said, I am also in the process of gaining further education in concussion. This is not your typical education about the injury but right were my mantra for the past six years has been:
The injury of concussion is not the true problem; it is the mismanagement of this brain injury that is the real issue.
As noted in March I began the Evidence in Motion Concussion Management Course. This is a 34 week program that was designed to bring collaboration and current information to those that can impact the real problem of this injury, the clinicians.
We have arrived at the half way point in the program, marked by the weekend intensive course – which met in Chicago this past weekend. Many have wanted to know has it been worth it. The answer is unequivocally, YES.
Before I get to the hands on of the weekend let me recap the first half of the program. One word cannot do it justice but in our search for snippets of information and quick reaction, that one word could be “trailblazing”.
Previously I wrote about how the program was basically going in terms of mechanics and what we were doing at the time. Since then I have read more research (current), discussed, and most importantly learned how to better help those that have been concussed.
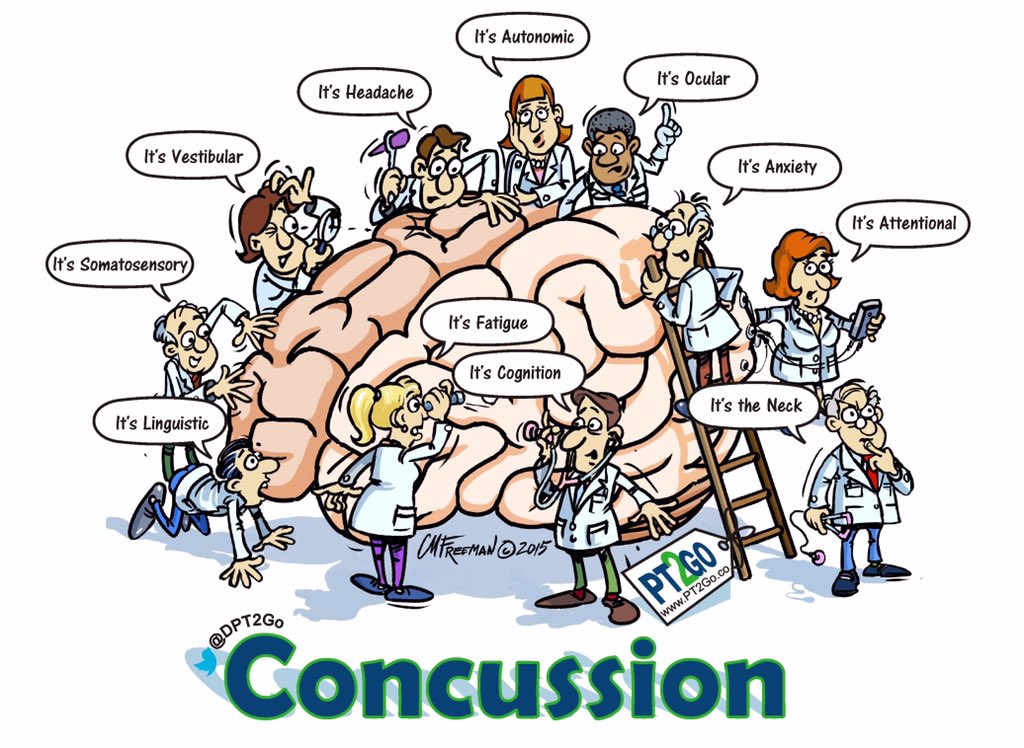
We finished the Therapeutic Neuroscience Education and moved into the specifics of the concussion and its management. We spent a week on each of the following parts of the concussion continuum:
- Emergency Department – evolution and how they view the injury
- Orthopedics – how concussion relates to bones and muscles (neck)
- Vestibular Rehab – not only the vestib system but really focusing on the eyes
- Adult/Migraines – a previously unthought of link/predisposition for concussion
- Vision Rehab – what I feel will be the next area of focus for recovery from concussion
- Neuropsych/Return to Learn – how we all fit together in these areas as clinicians
- Speech Language Pathology – unknown to me how these professionals can and will help
Those seven weeks, plus the last week of summary were probably the most challenging Continue reading
 The meeting at Georgetown University this past weekend was more than fruitful for this athletic trainer. I went in trying to get two things done: one, provide info to you the follower as best as possible and move along the discussion on female concussion and two, to learn something that is applicable to me as a “boot on the ground” athletic trainer.
The meeting at Georgetown University this past weekend was more than fruitful for this athletic trainer. I went in trying to get two things done: one, provide info to you the follower as best as possible and move along the discussion on female concussion and two, to learn something that is applicable to me as a “boot on the ground” athletic trainer. Concussion information is moving at a warp speed, it seems, compared to the long history of other medical issues that we face and hear about – cancer, heart disease, diabetes, etc. In fact, concussion is not an acknowledged speciality of the medical field, yet there are more and more monies and time being devoted to this current issue.
Concussion information is moving at a warp speed, it seems, compared to the long history of other medical issues that we face and hear about – cancer, heart disease, diabetes, etc. In fact, concussion is not an acknowledged speciality of the medical field, yet there are more and more monies and time being devoted to this current issue. What follows below are recommendations that have been on this blog for many years. I came up with them when it started in 2010 and not much has happened to change what was written. In fact, more and more these ideas have been accepted, showing that it was ahead of its time in 2010.
What follows below are recommendations that have been on this blog for many years. I came up with them when it started in 2010 and not much has happened to change what was written. In fact, more and more these ideas have been accepted, showing that it was ahead of its time in 2010. I just saw this on Twitter from @NSAFitness,
I just saw this on Twitter from @NSAFitness, 
 I trust everyone has had a wonderful Christmas experience (or Hanukkah or Kwanzaa or going to have a good Boxing Day), with that I would like to wish everyone continued successes in whatever endeavor they choose. Over the Holiday I have received many an email regarding concussions; apparently the down time has given people opportunity to share frustrations or good news.
I trust everyone has had a wonderful Christmas experience (or Hanukkah or Kwanzaa or going to have a good Boxing Day), with that I would like to wish everyone continued successes in whatever endeavor they choose. Over the Holiday I have received many an email regarding concussions; apparently the down time has given people opportunity to share frustrations or good news. One of the more gratifying things about this blog is the chance to educate anyone about concussions and the athletic training profession. I truly enjoy going out to speak and even debate this hot topic. I understand that my thought process is not like everyone else, nor do I expect everyone to see it the way I do; however I do want people to become more educated and understand what we are facing with this problem.
One of the more gratifying things about this blog is the chance to educate anyone about concussions and the athletic training profession. I truly enjoy going out to speak and even debate this hot topic. I understand that my thought process is not like everyone else, nor do I expect everyone to see it the way I do; however I do want people to become more educated and understand what we are facing with this problem. If you all recall I went to Zurich in November to attend the “Concussion Conference”; mainly as an observer, but there was enough time and opportunity to impart my questions/knowledge as a practicing athletic trainer. Here are the links to
If you all recall I went to Zurich in November to attend the “Concussion Conference”; mainly as an observer, but there was enough time and opportunity to impart my questions/knowledge as a practicing athletic trainer. Here are the links to 

 Time is short on this, I understand, but I just was dropped a note about this symposium being held in Chicago. Once again yours truly has “commitments”, this time it is a wrestling dual tournament – where my services are needed more. Regardless, when I looked at the faculty list and the speaking topics my interest was piqued. BIG NOTE here it is only $25 for athletic trainers to attend ($60 for physicians).
Time is short on this, I understand, but I just was dropped a note about this symposium being held in Chicago. Once again yours truly has “commitments”, this time it is a wrestling dual tournament – where my services are needed more. Regardless, when I looked at the faculty list and the speaking topics my interest was piqued. BIG NOTE here it is only $25 for athletic trainers to attend ($60 for physicians).
 This one is a very good seminar for anyone who deals with school aged children and once again it is free. This event will be put on by the CDC and the most poignant part is the academic and return to school concerns when dealing with the brain injury known as concussion. It has been my opinion that not only have the parents and schools underplayed the seriousness of returning to school with a brain injury, the medical community has been behind as well. Brain health will need to be though of as physical health going forward. Not only is stressing the cognitive parts of the brain while injured a problem, the most overlooked portion of school is something Don Brady has been the champion of, the emotional wellness of the brain/individual.
This one is a very good seminar for anyone who deals with school aged children and once again it is free. This event will be put on by the CDC and the most poignant part is the academic and return to school concerns when dealing with the brain injury known as concussion. It has been my opinion that not only have the parents and schools underplayed the seriousness of returning to school with a brain injury, the medical community has been behind as well. Brain health will need to be though of as physical health going forward. Not only is stressing the cognitive parts of the brain while injured a problem, the most overlooked portion of school is something Don Brady has been the champion of, the emotional wellness of the brain/individual.
 Some of the most important posts will be re-published from time to time. This one was published in October of 2010.
Some of the most important posts will be re-published from time to time. This one was published in October of 2010.